 NHSL Referral Pathways
NHSL Referral Pathways
- Evidence from digital rectal examination of a hard, irregular prostate
- Elevated or rising age-specific PSA. Rough guide to normal PSA levels (ng/ml):
- Less than 60 years < 3
- Aged 60-69 years < 4
- Aged 70-79 years < 5
These figures are a pragmatic aid based on clinical consensus. The principles of Realistic Medicine should be applied when considering referral and, in older men, routine or no referral may be appropriate for PSA levels of:
- Aged 80-85 years > 10
- Aged 86 years and over > 20
A PSA test may be raised within three days of ejaculation or six weeks of a proven UTI, catheterisation or other invasive procedure, such as prostate biopsy. 5 alpha reductase inhibitors such as finasteride may reduce the PSA level. Please refer men with more than one PSA to stratify whether referral should proceed along a cancer pathway or otherwise. It should be noted that the majority of men with prostate cancer have no symptoms at all.
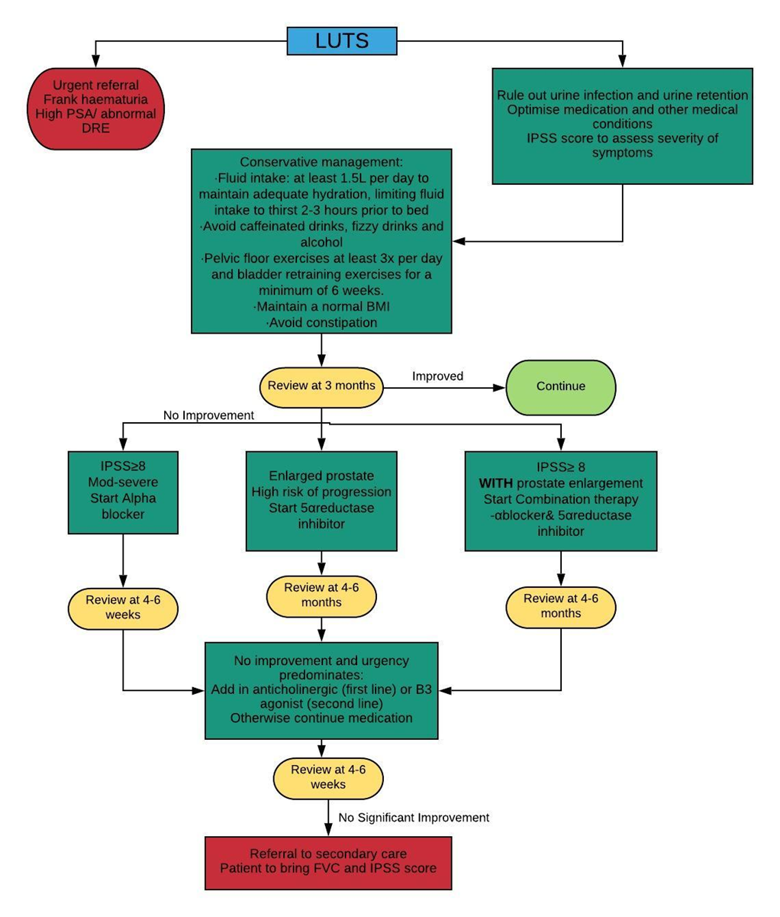
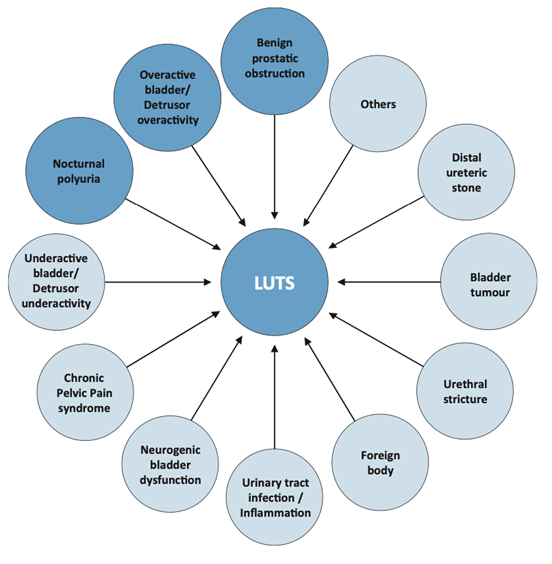
Initially, a urine infection and urinary retention should be ruled out and other medical conditions or medications which result in LUTS should be optimised e.g. diabetes, cardiac failure, renal failure and neurological conditions.
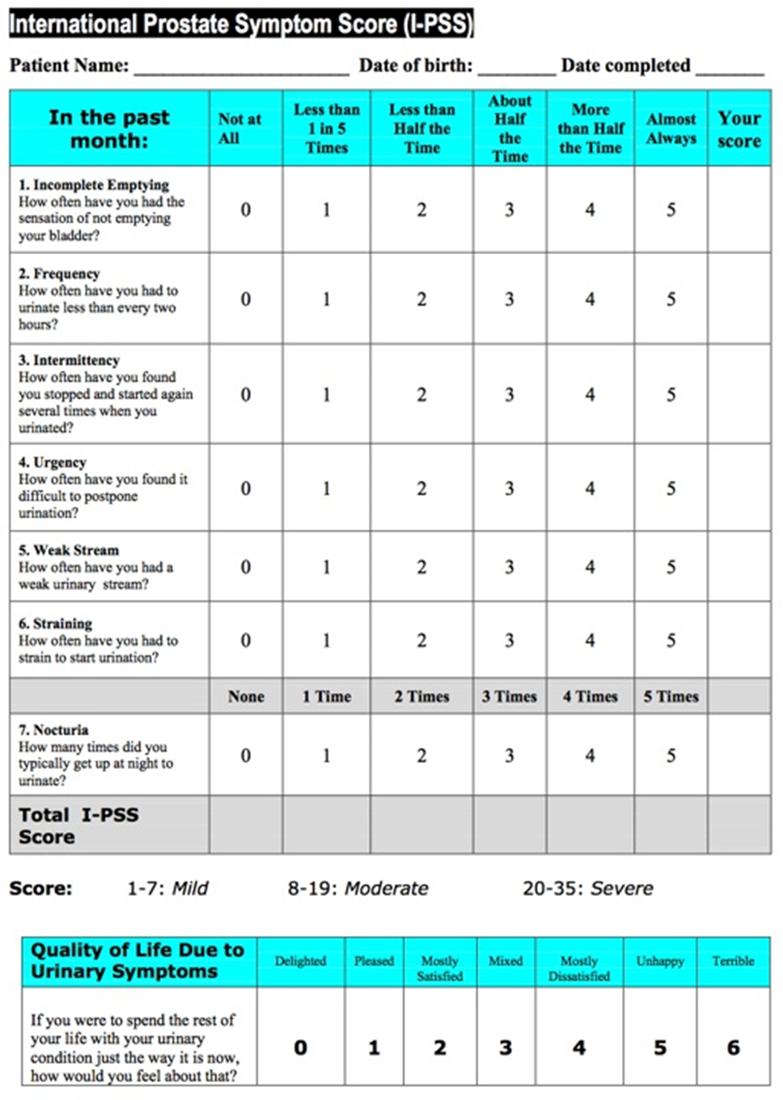
The severity of LUTS and response to treatment is categorised using the International Prostate Severity Scoring (IPSS) tool (see below). Many patients can be managed in the community with the following recommendations from NICE and European Association of Urology (EAU) guidelines.